Mortality and morbidity drivers of international health inequality

Over the last decades, survival prospects have generally increased worldwide. Using data from the Global Burden of Disease project, Iñaki Permanyer and Octavio Bramajo investigate how mortality and morbidity have affected the levels and changes in “International Health Inequality” (i.e., variability in the distribution of life expectancies across countries).
We know a lot about countries’ generalized improvements in life expectancy, or LE (Riley 2015), but much less is known about international variability in LE and its drivers over time. Are LE levels in countries across the world becoming increasingly similar or dissimilar over time? To what extent are these trends driven by changes in the number of years individuals survive in “good” or in “less-than-good” health? In a recently published study (Permanyer and Bramajo 2023) we address these fundamental research questions, which have profound implications for the global development agenda and the sustainability of welfare and care systems in an ageing world.
The race between mortality and morbidity
Assessments of longevity and its variability in countries around the globe are often based on life expectancy but tend not to differentiate between years spent in “good” or “less-than-good” health. Depending on the relative speeds at which the occurrence of mortality and the onset of morbidity are delayed (the “race between mortality and morbidity”), the average number of years individuals can expect to live in “good health” (also known as Health-adjusted Life Expectancy, or HALE) or in “less-than-good health” (Unhealthy Life Expectancy, or UHLE) can differ dramatically. These morbi-mortality dynamics have consequences for
1- the composition of countries’ LE in its healthy and unhealthy components, and
2 – the extent of inequality in LE between countries, henceforth denoted as “International Health Inequality”, or IHI.
Figure 1 shows the joint evolution of HALE and UHLE across 204 countries and territories between 1990 and 2019 using estimates from the Global Burden of Disease (GBD) project. Despite a few exceptions, the values of HALE and UHLE tend to increase simultaneously over time, although at different speeds. The United States stands out as a clear outlier, with UHLE increasing at the fastest rate. In general, in the countries that were more longevous in 1990 (with higher LE), the contribution of the HALE component to further increases in LE decreased over time. Graphically, the arrows starting at high LE levels tend to be shorter and have steeper slopes.
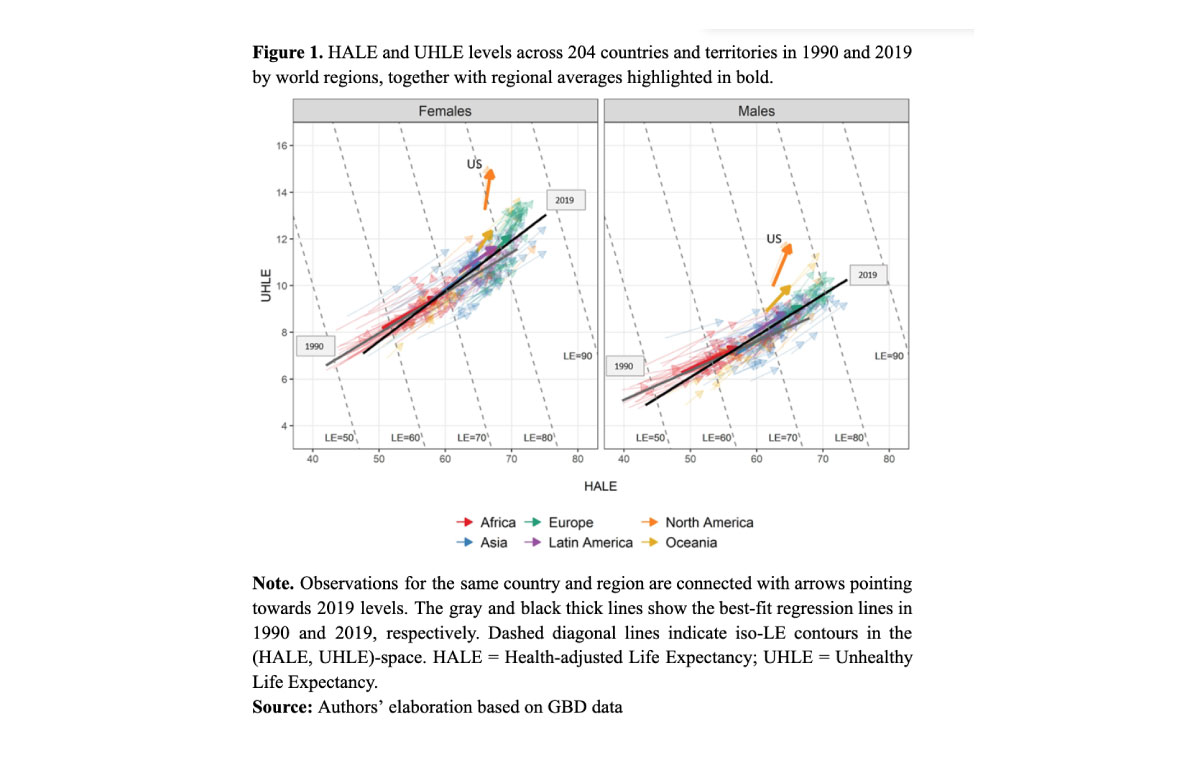
The slope of the best-fitting regression line tends to increase when moving from 1990 (gray line) to 2019 (black line), both for women and men. Likewise, the best-fit regression line for women has a higher slope than that of men, both in 1990 and 2019. This suggests that the contribution of UHLE to LE has increased over time and is greater among women. The relative position of the clouds of points in the two panels of Figure 1 confirms that, at any fixed level of LE (say 60, 70, 80 years), men spend a larger fraction of their lives in good health than women.
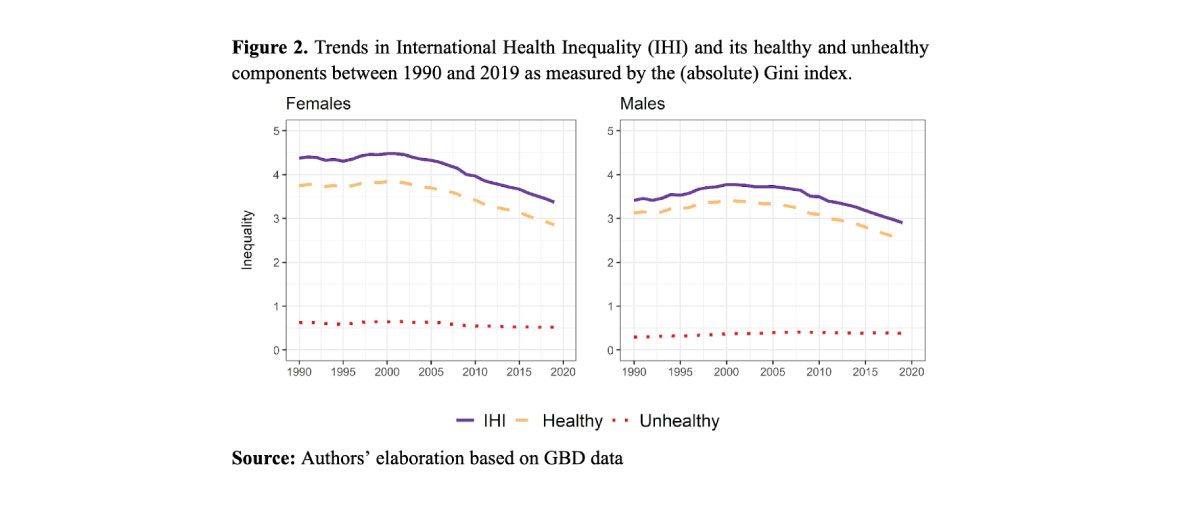
Figure 2 shows levels of IHI as measured by the (absolute) Gini index, a popular index of inequality measuring the expected difference in LE between two randomly chosen countries. For women, IHI hovered around 4.4 years until the early 2000s, and then started declining monotonically, approaching 3.37 in 2019. For men, IHI increased between 1990 and 2000 from 3.41 to 3.77 years and then started declining to reach its minimum of 2.9 in 2019.
Figure 2 also shows the contributions of HALE and UHLE to IHI. As can be seen, IHI values are mostly explained by variations of HALE across countries. In contrast, the contribution of cross-country variations in UHLE to IHI remained relatively flat during the observation period, at some 0.5 years, but this also means that the fraction of IHI attributable to cross-country variations in UHLE has increased over time, especially for men.
Discussion and conclusions
Our findings indicate that IHI levels are mostly explained by variations in HALE across countries, so attempts at curbing IHI should be directed towards increasing HALE for the countries at the bottom of the “healthy longevity distribution”, primarily through disease prevention and improvements in the socio-economic environment. Conversely, treating chronic diseases or disability tends to expand UHLE.
Global health inequalities are undergoing profound transformations. On the one hand, inequality in life expectancy between countries has resumed its downward trend after the temporary blip in the 1990s prompted by the spread of the HIV-AIDS epidemic in Sub-Saharan Africa and the collapse of the Soviet Union (Goesling and Firebaugh 2004). At the same time, there is increasing evidence that health inequalities within countries are strong and persistent, very often in relation to socioeconomic status (Zazueta et al 2023). While still relevant, country of residence is gradually losing prominence as a determining factor of individual survival prospects.
On the other hand, morbidity onset is playing an increasingly important role in explaining both improved survival prospects among longevity vanguard countries and longevity differences between world countries. As longevity increases further, mortality-related inequalities will be primarily disease- and disability-centered (Permanyer et al 2023). Therefore, interventions to improve population health should increasingly focus on the health “disorders that debilitate, rather than kill” (Murray et al 2015, p. 38). In the coming decades, the aforementioned transformations will shape the contours of the research agenda and interventions among scholars and policy-makers concerned with global health inequalities.
References
Goesling, Brian and Firebaugh Glenn. 2004. “The Trend in International Health Inequality.” Population and Development Review 30(1): 131–146. https://doi.org/10.1111/j.1728-4457.2004.00006.x
Murray, Christopher J.L., Ryan M. Barber, Kyle J. Foreman, Ayse Abbasoglu Ozgoren, Foad Abd-Allah, Semaw F. Abera, Victor Aboyans., et al. 2015. “Global, Regional, and National Disability-Adjusted Life Years (DALYs) for 306 Diseases and Injuries and Healthy Life Expectancy (HALE) for 188 Countries, 1990–2013: Quantifying the Epidemiological Transition.” The Lancet 386 (10009): 2145–2191. https://doi.org/10.1016/S0140-6736(15)61340-X.
Permanyer, Iñaki and Octavio Bramajo. 2023. “The race between mortality and morbidity: Implications for the global distribution of health”, Population and Development Review. https://doi.org/10.1111/padr.12582.
Permanyer, Iñaki, Francisco Villavicencio and Sergi Trias-Llimós. 2023. “Healthy lifespan inequality: Morbidity compression from a global perspective.” European Journal of Epidemiology 38(5): 511–521. https://doi.org/10.1007/s10654-023-00989-3.
Riley, James C. 2015. Rising Life Expectancy: A Global History. Cambridge University Press. https://doi.org/10.1017/CBO9781316036495.
Zazueta-Borboa JD, Martikainen P, Aburto JM, et al. 2023. “Reversals in past long-term trends in educational inequalities in life expectancy for selected European countries”, Journal of Epidemiology & Community Health; 77:421-429.
Source figure 1 and 2 – Authors’ elaboration based on GBD data