Frailty at death: A four-country study

Frailty represents a major public health challenge in ageing populations. In this study, Sergi Trias-Llimós, Magali Barbieri, Viviana Egidi, Luisa Frova, Francesco Grippo, France Meslé, Marilena Pappagallo, and Aline Désesquelles focus on frailty at death in people aged 50 years and above in France, Italy, Spain and the US.
The continuous decline in mortality among the elderly, except during the COVID-19 period, has contributed to increased population heterogeneity with respect to frailty, “a state of increased vulnerability to poor resolution of homeostasis after a stressor event, which increases the risk of adverse outcomes” (Clegg et al., 2013). In ageing populations, frailty represents a major public health challenge because of both its increasing prevalence over time and its association with mortality risks.
Understanding the role of frailty, in part(s)
In a recent study, we examined the distribution of frailty-related causes mentioned on death certificates in France, Italy, Spain and the United States in 2017 (Trias-Llimós et al., 2023). Death certificates, usually completed by physicians, provide information on the morbid process, including the sequence of diseases and conditions leading to death (in Part I of the certificate) and the contribution of other causes, not directly involved (in Part II). Most studies of mortality by cause rely on the underlying cause of death, which is the disease or injury that initiated the train of events leading to death. Whereas this information is undoubtedly of value, it limits the understanding of mortality processes and the role played by the diseases (conditions, or risk factors) that are rarely designated as the initial cause.
We defined a list of frailty-related causes of death by adapting the list in Soong et al. (2015), including dementia, incontinence, functional dependence and mobility problems, decubitus ulcer and pressure area, and senility. We excluded falls and fractures, which are causes or consequences of frailty rather than frailty per se, and anxiety and depression; and we added malaise, fatigue and malnutrition, types of vulnerabilities that are rarely listed as underlying causes of death (Grippo et al. 2020). If mentioned in Part I, they likely correspond to end-of-life symptoms and do not necessarily reflect pre-existing frailty in the deceased. If mentioned in Part II, they indicate vulnerability and are more likely to reflect pre-existing conditions which could have increased the risk of dying from the underlying cause.
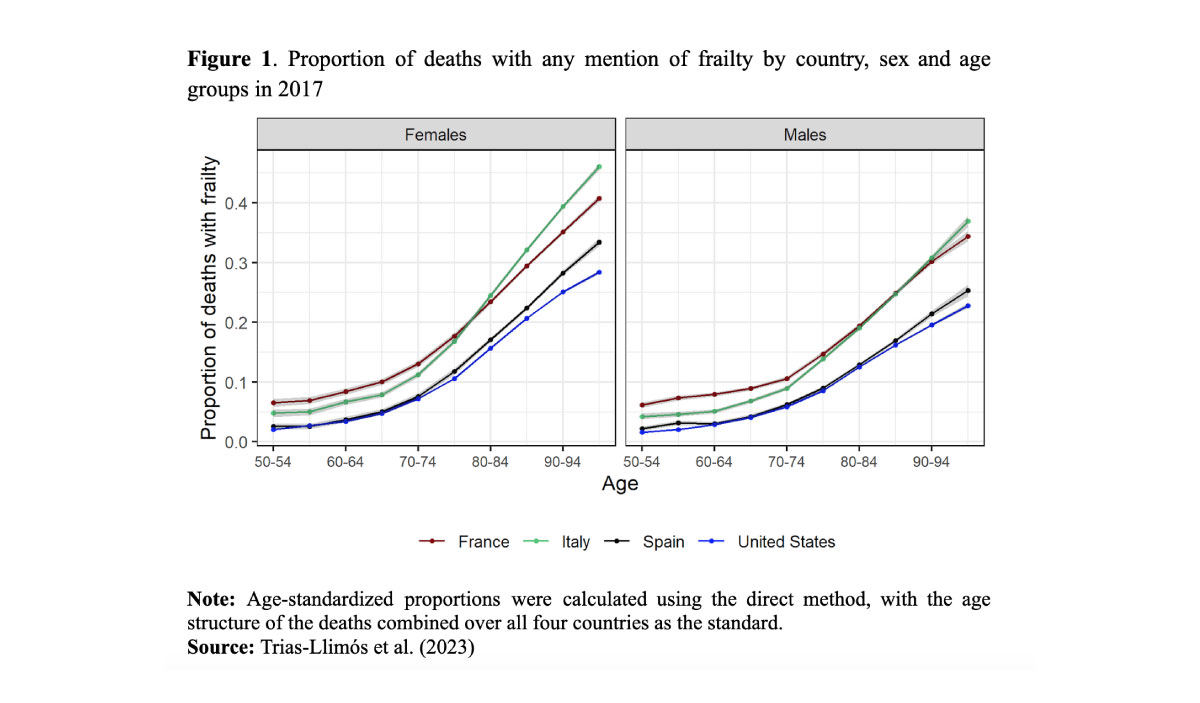
Overall, the age-standardized proportion of deaths with frailty at 50 years and over was highest in Italy (24.4%), followed by France (22.7%) and Spain (16.6%), and lowest in the US (14.9%). The proportion of death certificates with a mention of frailty increases with age for both sexes across the four countries (Figure 1). It is highest in France and lowest in Spain and the US at younger ages, and highest in Italy at older ages. The share of deaths with a mention of frailty is higher for women than for men across all countries and age groups, with a mean female to male ratio of 1.21.
In all four countries, frailty mentions are most frequent in Part I, although not as the underlying causes of death, for which large cross-country differences are observed, with high proportions in Italy and France, and low proportions in the US and Spain. Conversely, when a frailty-related condition is mentioned as either the underlying cause of death or in Part II, cross-country differences become small.
Where frailty is mentioned
Figure 2 shows the distribution of frailty mentions according to their position on the death certificate (as the underlying cause, elsewhere in Part I, or in Part II) by country, age, and sex. Dementia is the most common frailty-related cause mentioned as the underlying cause in all countries and for both sexes, with the exception of the 50-64 year age group in France, for whom cachexia and protein-energy malnutrition are more prevalent. The cause-of-death distribution is substantially different if we look at frailty listed in Part I but not as the underlying cause. Dementia remains the most prevalent cause in Spain and the US, but cachexia and protein-energy malnutrition represent an important share (at least 25% of the deaths with frailty mentioned in Part I at ages 50-64 years). Malaise and fatigue are also reported in at least 25% of certificates in France, while the prevalence of mobility problems and senility increases with age (e.g., 50% of deaths at ages 80 years and over in Italy).
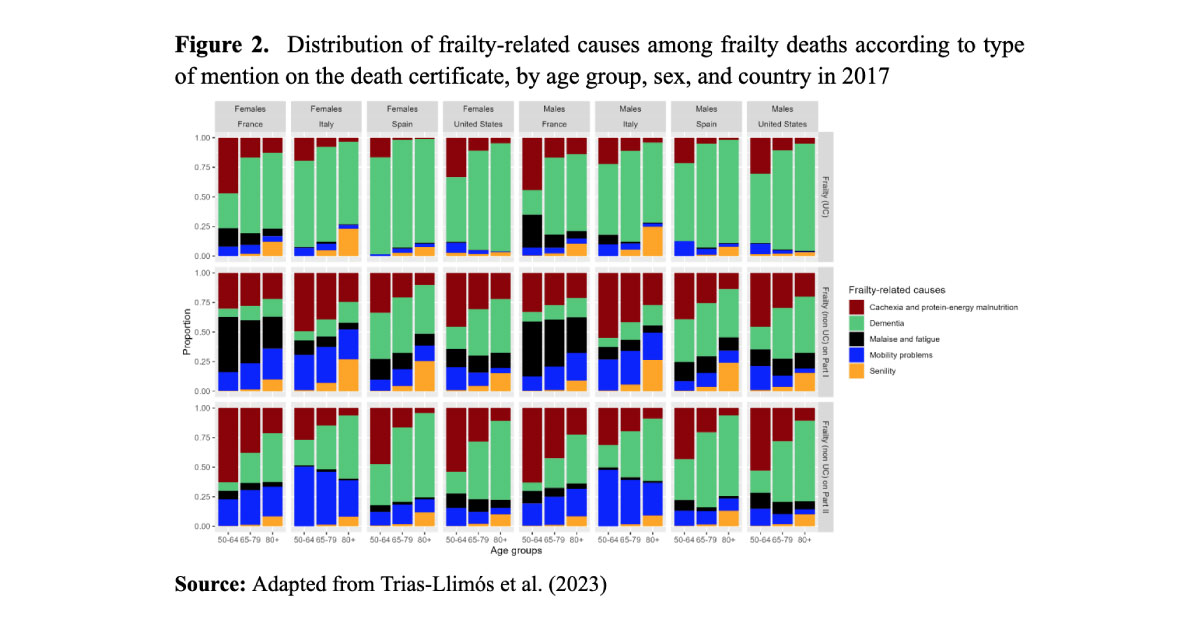
Finally, when frailty is mentioned in Part II, dementia is again the most commonly reported condition, followed by cachexia and protein-energy malnutrition and senility. Strong age patterns are found: while the share of dementia mentions increases with age, the share of mentions of cachexia and protein-energy malnutrition declines.
Conclusions
Our study provides a basis for further monitoring of frailty in low-mortality countries using a widely available and highly comparable source of information. Frailty might be underreported by certifying physicians, either because they consider almost everyone to be frail at the end of life, especially at more advanced ages, or because frailty syndromes are not considered as valid causes of death, so our estimates are likely to be conservative. However, the consistency of our results by sex and over the age curve appears to reflect plausible patterns indicating real differences in the prevalence of frailty at the end of life.
References
Clegg, A., Young, J., Iliffe, S., Rikkert, M. O., & Rockwood, K. (2013). Frailty in elderly people. The Lancet, 381(9868), 752–762.
Fried, L. P., Tangen, C. M., Walston, J., Newman, A. B., Hirsch, C., Gottdiener, J., Seeman, T., Tracy, R., Kop, W. J., & Burke, G. (2001). Frailty in older adults: Evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56(3), M146–M157.
Grippo, F., Désesquelles, A., Pappagallo, M., Frova, L., Egidi, V., & Meslé, F. (2020). Multi-morbidity and frailty at death: A new classification of death records for an ageing world. Population Studies, 74(3), 437–449.
Soong, J., Poots, A. J., Scott, S., Donald, K., Woodcock, T., Lovett, D., & Bell, D. (2015). Quantifying the prevalence of frailty in English hospitals. BMJ Open, 5(10), e008456. https://doi.org/10.1136/bmjopen-2015-008456
Trias-Llimós, S., Barbieri, M., Egidi, V., Frova, L., Grippo, F., Meslé, F., Pappagallo, M., & Désesquelles, A. (2023). Frailty at death: An examination of multiple causes of death in four low mortality countries in 2017. Demographic Research, 49(2), 13–30.